
The Danger of Rushing Hair Growth: Why Controlling Hair Fall Must Come First in Alopecia Areata
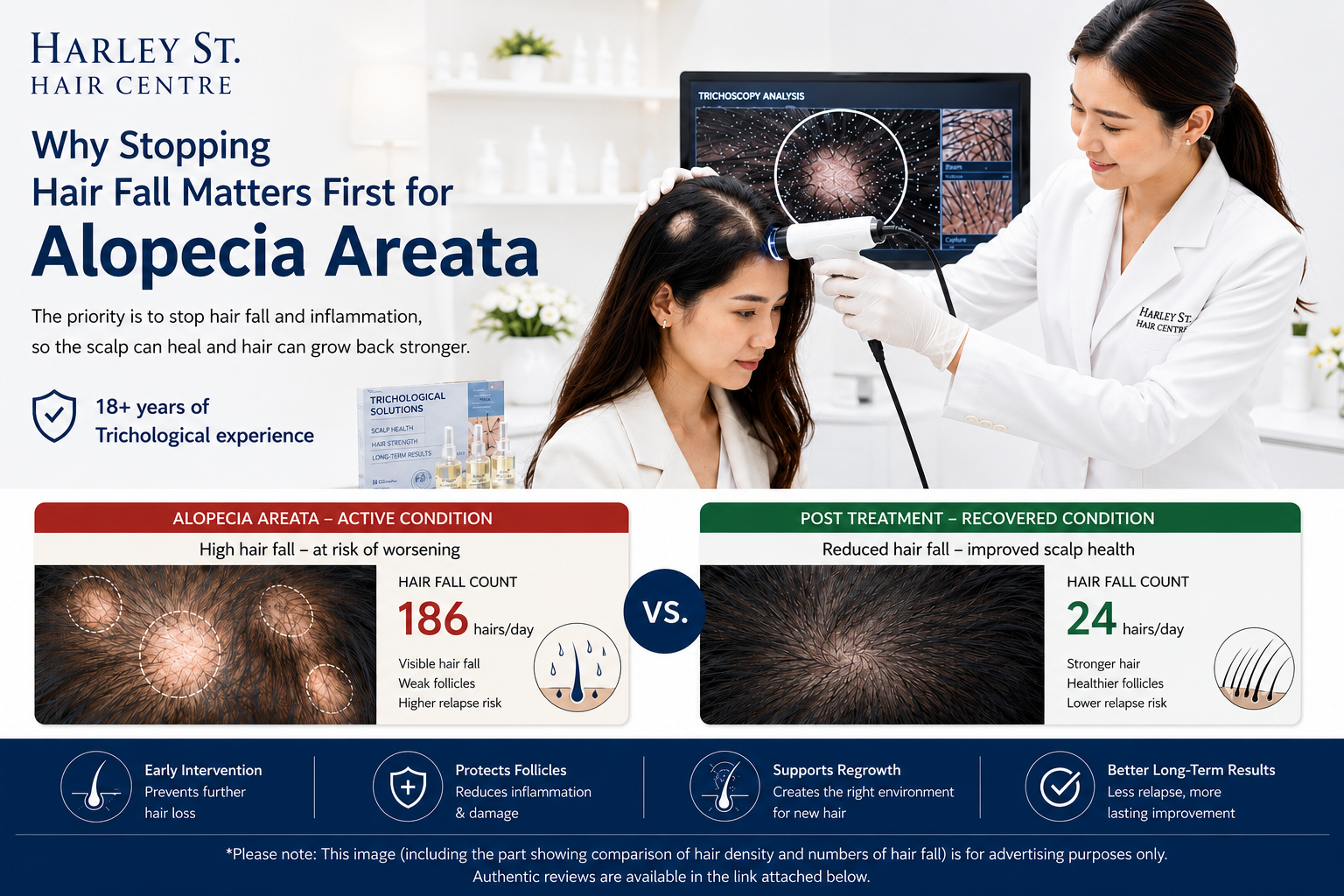
Hair and scalp specialist at Harley St. Hair Centre performing a Trichoscopy Analysis for Alopecia Areata, with a comparison of hair fall count and hair density before and after supportive hair care.
Discovering a sudden, smooth bald patch on your scalp can be terrifying. For individuals diagnosed with Alopecia Areata, the immediate instinct is often a frantic rush to regrow the missing hair. However, jumping straight into aggressive hair growth treatments without first stabilizing acute, rapid shedding is a counter-productive strategy that frequently ends in clinical frustration. This article breaks down the complex biological landscape of Alopecia Areata and explains why a British-vetted, Trichological approach focusing on stabilizing the scalp ecosystem yields far more sustainable, safer results than standard, aggressive growth stimulants.
The Fatal Flaw of Forcing Growth in an Active Immune Battlefield
Alopecia Areata (AA) is fundamentally an autoimmune condition, meaning the body’s immune system mistakenly targets its own hair follicles, plunging them into a premature shedding phase [Pratt et al., 2017]. When a scalp is in an active state of acute shedding, forcing dormant follicles to produce new hair via aggressive growth stimulants is akin to planting seeds in a burning forest.
The standard medical playbook often relies heavily on :
Systemic or Intralesional Corticosteroids: High-potency steroid injections or creams designed to suppress localised inflammation [Almohanna et al., 2019].
Aggressive Growth Stimulants & Hormonal Agents: Medications like topical or oral Minoxidil, Finasteride, or Dutasteride [Vano-Galvan et al., 2021].
While these conventional pharmaceutical interventions can trigger rapid, forced hair sprouting, they fail to correct the underlying structural vulnerability of the hair follicle or the disrupted scalp environment [Strazzulla et al., 2018]. Minoxidil, for example, is a vasodilator that forces blood flow to the follicle to accelerate growth, but it possesses absolutely zero mechanisms to halt an ongoing autoimmune attack [Ubie Health, 2025].
Consequently, any new hair forced to grow under this high-pressure pharmaceutical environment lacks a stable anchor. Before these fragile strands can mature, develop a strong cortex, or contribute to genuine, long-term hair density, the underlying inflammation cuts them down, causing them to shed prematurely [MIMS Thailand, 2026].
The Severe Rebound Effect: When Aggressive Treatments Fire Back
One of the most distressing realities for Alopecia Areata patients undergoing standard medical treatments is the high prevalence of the rebound effect. Because corticosteroids and powerful growth stimulants merely mask inflammation or force temporary follicular activity, stopping the treatment—or even maintaining it as the body develops a tolerance—can cause the underlying autoimmune response to return with a vengeance [National Alopecia Areata Foundation, 2021].
Clinical case studies consistently show that when the temporary suppression from steroids or strong pills wears off, patients often suffer from a dramatic recurrence [American Academy of Dermatology, 2024]. Not only do the original balding spots return, but they frequently reappear larger, more aggressive, or multiply across the scalp.
Unlike standard male or female pattern hair loss, which progresses slowly over decades, Alopecia Areata is highly unpredictable and volatile. If the follicular structure is repeatedly shocked by cycling through aggressive growth phases followed by sudden, severe immune-mediated shedding, it can lead to permanent follicular scarring and irreversible destruction of the hair root [Zhou et al., 2023]. In the most severe instances, this cyclical trauma accelerates patchy Alopecia Areata into terminal, widespread variants :
Alopecia Totalis: The complete loss of all hair on the entire scalp [Pratt et al., 2017].
Alopecia Universalis: The total loss of all hair across the entire scalp and body [Pratt et al., 2017].
This rapid deterioration can occur in just a few months when the immune system becomes completely destabilized by aggressive, short-term pharmaceutical cycling [National Alopecia Areata Foundation, 2021].
The Trichological Alternative: A British Approach to Scalp Ecosystem Recovery
This divergence in patient outcomes does not occur because dermatologists lack skill; rather, it stems from a fundamental difference in clinical focus. Conventional dermatology is primarily trained to manage acute skin diseases through rapid, symptom-masking pharmaceutical suppression. Conversely, the science of Trichology—which originated and was formalised in the United Kingdom—views hair loss through the lens of holistic, long-term ecosystem restoration.
UK-trained Trichologists do not treat Alopecia Areata with aggressive, volatile synthetic hormones or localized steroid injections. Instead, they champion a safer, non-invasive methodology that prioritizes two critical phases :
Phase 1 : Anti-Hair Loss Control & Inflammation Reduction
Before a single strand of hair is encouraged to grow, the primary objective is to dramatically decrease the daily rate of hair fall. By utilising personalised, gentler topical treatments specifically engineered to calm the localised micro-environment, Trichologists work to establish a defensive barrier around the follicle, effectively shielding it from ongoing immune irritation.
Phase 2 : Follicular Rehabilitation & Scalp Function
Once abnormal shedding is controlled, treatment shifts toward rebuilding the health of the hair follicle and restoring natural scalp function. This bespoke approach ensures that when the hair follicle naturally transitions back into its growth phase (anagen), it does so within a clean, balanced, and structurally sound environment. The resulting hair strands are strong, deeply rooted, and capable of achieving maximum density without the risk of a sudden pharmaceutical crash.
Proven Recovery: Harley St. Hair Centre in Bangkok
Bringing the elite standards of British Trichology to Thailand, Harley St. Hair Centre in Bangkok has spent over 18 years successfully treating complex, volatile cases of Alopecia Areata in both adults and young children.
Many of the centre's most successful client recovery stories come from individuals who previously sought treatment through strong dermatological drugs, only to experience severe side effects, scalp thinning, or devastating rebound spots. By pivoting to the personalised, non-surgical, and steroid-free topical programs developed under British trichological expertise, these clients managed to stop active shedding, safely restore their natural hair density, and protect their scalps from permanent scarring..
By treating the hair root as a delicate living organ rather than a symptom to be forced, sustainable, side-effect-free recovery from Alopecia Areata is entirely possible.
Medical References :
Almohanna, H. M., Ahmed, A. A., Tsatalis, J. P., & Tosti, A. (2019). Systemic Corticosteroids in the Treatment of Alopecia Areata: A Systematic Review. Dermatology and Therapy, 9(2), 259-270.American Academy of Dermatology (AAD). (2024). Hair loss types: Alopecia areata diagnosis and treatment. Retrieved from AAD Guidance Documents.MIMS Thailand. (2026). Alopecia : Clinical Management and Corticosteroid Protocols. MIMS Disease Management Directory.National Alopecia Areata Foundation (NAAF). (2021). Available Treatments and Follicular Mechanics in Patchy Alopecia. NAAF Patient & Clinical Toolkit.Pratt, C. H., King, L. E., Messenger, A. G., Christiano, A. M., & Sundberg, J. P. (2017). Alopecia areata. Nature Reviews Disease Primers, 3(1), 1-17.Strazzulla, L. C., Wang, E. H., Avila, L., Lo Sicco, K., Brinster, N., Christiano, A. M., & Shapiro, J. (2018). Alopecia areata: Disease characteristics, clinical evaluation, and new perspectives on pathogenesis. Journal of the American Academy of Dermatology, 78(1), 1-12.Ubie Health. (2025). Does minoxidil help alopecia areata? Clinical Insights and Off-Label Limitations. Ubie Doctor's Note Series.Vano-Galvan, S., Pirmez, R., Hermosa-Gelbard, A., & Saceda-Corralo, D. (2021). Safety and effectiveness of oral minoxidil for severe and patchy alopecia areata. Journal of the European Academy of Dermatology and Venereology, 35(11), e735-e737.Zhou, C., Li, X., Wang, C., & Zhang, J. (2023). Follicular Scarring and the Risk of Progression to Alopecia Totalis in Uncontrolled Autoimmune Shedding. International Journal of Molecular Sciences, 24(8), 6901.